Although CPT code 99214 is one of the most frequently used codes for outpatient Evaluation and Management (E/M) services across the United States of America (USA), it also stands as one of the most commonly misunderstood and misused. When handling these claims, medical practices must stay vigilant to maintain compliance and avoid audit risks.
When does an encounter truly meet the threshold of moderate complexity? How exactly should your clinical team document it? What compliance shifts occur when the visit is conducted via telehealth? These lingering questions often turn into small administrative doubts that ultimately result in undercoding, overcoding, or costly medical billing rejections. You can learn more about managing these billing errors by reviewing our guide on co-45 denial code what it means and how to handle it.
This comprehensive guide breaks down everything you need to know. You will master how to properly code an established outpatient visit, understand the stringent time and Medical Decision-Making (MDM) frameworks, correctly apply critical modifiers like the 25 modifier description, and ensure that every single claim accurately reflects the extensive care your practice delivers. For comprehensive operational support, consider checking out the reliable general practice medical billing services by MedicureMD.
Need Expert Guidance?
If your practice is struggling with E/M coding accuracy, compliance audits, or persistent claim denials, our specialized team is here to help optimize your revenue cycle.
What is CPT Code 99214 in Medical Coding?
CPT code 99214 is a level-4 Evaluation and Management (E/M) code designated for the evaluation and treatment of an established patient in an office or outpatient setting. In everyday clinical practice, this represents a visit where the healthcare provider is managing multiple chronic conditions, addressing an acute illness with systemic symptoms, or dedicating a significant block of time to the patient’s care. Accurate reporting here is standard practice across specialized fields like internal medicine.
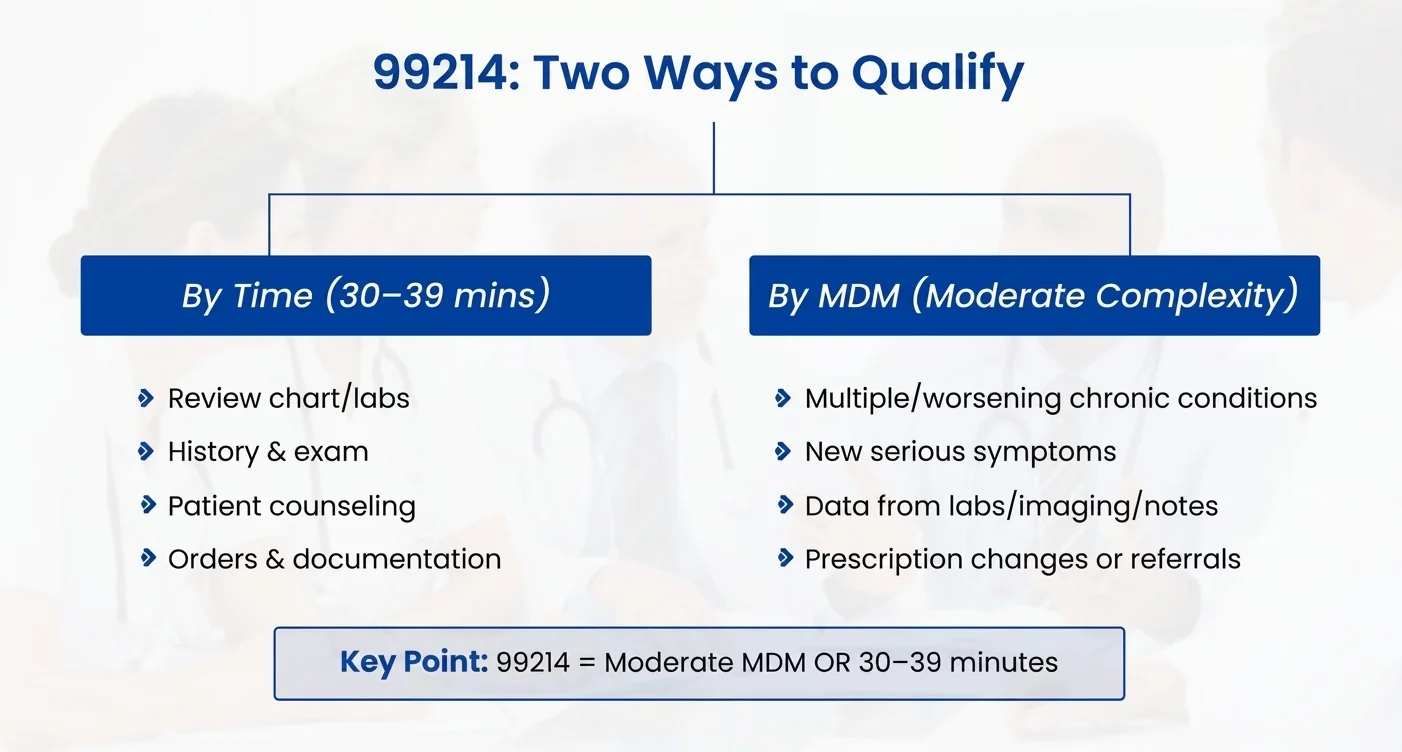
Per the guidelines established by the American Medical Association (AMA), a provider can determine and select a 99214 level of service based on one of two distinct criteria:
1. Medical Decision-Making (MDM)
The patient’s clinical presentation and the provider’s management plan must reach a moderate level of complexity. This means the clinician is managing at least two stable chronic conditions, evaluating one worsening chronic condition, reviewing diagnostic data from external sources, or managing inherent treatment risks that demand advanced clinical judgment. This structured approach ensures accuracy in general clinical care and specialized family medicine billing.
2. Time
The provider must document that they spent a total of 30 to 39 minutes of continuous or non-continuous care on behalf of that specific patient on the exact date of the encounter. This tracking encompasses both face-to-face time and non-face-to-face work performed on that calendar day. Failing to document this properly often results in preventable issues, similar to those explained in our resource on the co-45 denial code what it means and how to handle it.
Positioned strategically between routine, lower-level follow-up visits (CPT 99213) and highly complex, critical encounters (CPT 99215), the 99214 code captures visits that require deeper cognitive analysis, extensive data synthesis, and structured risk mitigation. Utilizing reliable general practice medical billing services by MedicureMD helps practices navigate these thresholds safely.
Typical Characteristics of a 99214 E/M Encounter
An office visit qualifies for a 99214 designation when the clinical workload or patient acuity naturally scales to a moderate complexity level. This occurs frequently across primary care specialties. For instance, detailed documentation of these factors is essential to ensure seamless reimbursement in family medicine billing, where chronic care is frequently managed.
The following clinical archetypes typically justify this coding level:
1. Management of Multiple Chronic Illnesses
When an established patient presents with two or more stable chronic conditions that require ongoing evaluation, systemic monitoring, or therapeutic adjustments, the cognitive load increases. This scenario represents the cornerstone of standard outpatient internal medicine care. Examples include:
- Type 2 Diabetes Mellitus combined with Essential Hypertension.
- Chronic Obstructive Pulmonary Disease (COPD) paired with Chronic Heart Failure.
- Stage 3 Chronic Kidney Disease (CKD) presenting alongside poorly controlled Diabetes.
2. New Medication Adjustments and Prescription Risk
Initiating a new prescription regimen, titrating current dosages, or implementing a high-risk therapeutic course drastically shifts the medical risk profile. Ensuring that your medical records clearly highlight these shifts protects your revenue stream from contractual write-offs, which we discuss in our breakdown of the co-45 denial code what it means and how to handle it.
Examples include:
- Beginning a new course of an antidepressant or mood stabilizer.
- Adjusting an insulin regimen based on erratic blood glucose logs.
- Modifying long-term anti-hypertensive medications or starting a systemic steroid taper.
3. New Undiagnosed Symptoms with a Serious Prognosis
When a patient presents with a novel, undiagnosed symptom that carries a high risk of morbidity if left untreated, the differential diagnosis process demands moderate MDM. Practices can rely on reliable general practice medical billing services by MedicureMD to format these acute claims properly.
Examples include:
- New-onset chest pain upon exertion.
- Unexplained neurological symptoms (intermittent numbness, localized weakness, or severe dizziness).
- Acute abdominal pain presenting with clinical “red-flag” indicators.
MDM vs. Time: The Two Pathways to 99214 Selection
Modern E/M guidelines decouple the final code selection from the traditional counting of history elements and physical examination bullets. While a medically appropriate history and physical exam must be performed and documented, they no longer dictate the final billing tier. Instead, providers have two clear pathways to achieve a CPT Code 99214, whether practicing in general wellness clinics or specialized internal medicine facilities:
| Selection Basis | Core Requirement for CPT 99214 |
| Medical Decision-Making | Must satisfy at least two out of three MDM elements: Moderate number/complexity of problems, Moderate volume/complexity of data, or Moderate risk of complications/morbidity. |
| Total Time | Exactly 30 to 39 minutes spent on the date of the encounter, explicitly documented in the medical record. |
What Counts Toward “Total Time”?
If you select your code based on time, you can accumulate all minutes personally spent by the billing provider on that specific calendar day. Tracking this thoroughly is an excellent habit to develop in family medicine billing workflows. This time includes:
- Reviewing historical charts, external imaging, and laboratory trends prior to entering the examination room.
- Obtaining the interval history and performing the physical examination.
- Counseling the patient, family members, or caregivers on treatment options.
- Ordering diagnostic tests, labs, or new prescription medications.
- Coordinating care with external specialists or community resources.
- Completing the electronic health record (EHR) clinical documentation after the patient leaves.
Proper Documentation Example: “I spent a total of 34 minutes reviewing past records, examining the patient, formulating the updated treatment plan, and documenting this encounter on today’s date.” Missing these explicit structural statements can generate audit red flags and lead to an unexpected co-45 denial code what it means and how to handle it.
Deconstructing Moderate MDM for CPT 99214
To secure a 99214 based on Medical Decision-Making, your documentation must clearly establish moderate complexity across at least two of the following three pillars. Outsourcing this validation to the team at reliable general practice medical billing services by MedicureMD ensures that compliance standards are always maintained.
Pillar 1: Number and Complexity of Problems Addressed
The clinical record must demonstrate that the provider actively evaluated and managed conditions requiring significant medical oversight. This includes managing 2 stable chronic illnesses, 1 chronic illness experiencing an acute exacerbation or progression, or 1 new acute illness presenting with systemic symptoms.
Pillar 2: Amount and/or Complexity of Data to be Reviewed
Data review becomes moderate when the provider synthesizes information across multiple domains. This is established by ordering or reviewing tests from at least three unique categories, or by independently interpreting an image or test performed by another provider. This level of cross-analysis is highly common inside advanced internal medicine environments.
Pillar 3: Risk of Complications and/or Morbidity of Patient Management
This is driven by the decisions made regarding treatment interventions. The absolute benchmark for moderate risk in daily practice is prescription drug management. This includes deciding to continue, stop, or alter a prescription medication due to potential side effects or therapeutic efficacy.
Common Clinical Scenarios Justifying CPT 99214
To bridge the gap between coding theory and practice, let’s look at three standard scenarios regularly encountered by clinics optimized through reliable general practice medical billing services by MedicureMD:
Scenario 1: Multi-System Chronic Disease Follow-Up
A 58-year-old established patient returns for routine monitoring of Type 2 Diabetes, Hypertension, and Stage 3 CKD.
- Problems Addressed: Three chronic, co-morbid conditions requiring systemic oversight (Moderate).
- Data Reviewed: The provider reviews a recent basic metabolic panel, eGFR trends, and an external nephrology consultation note (Moderate).
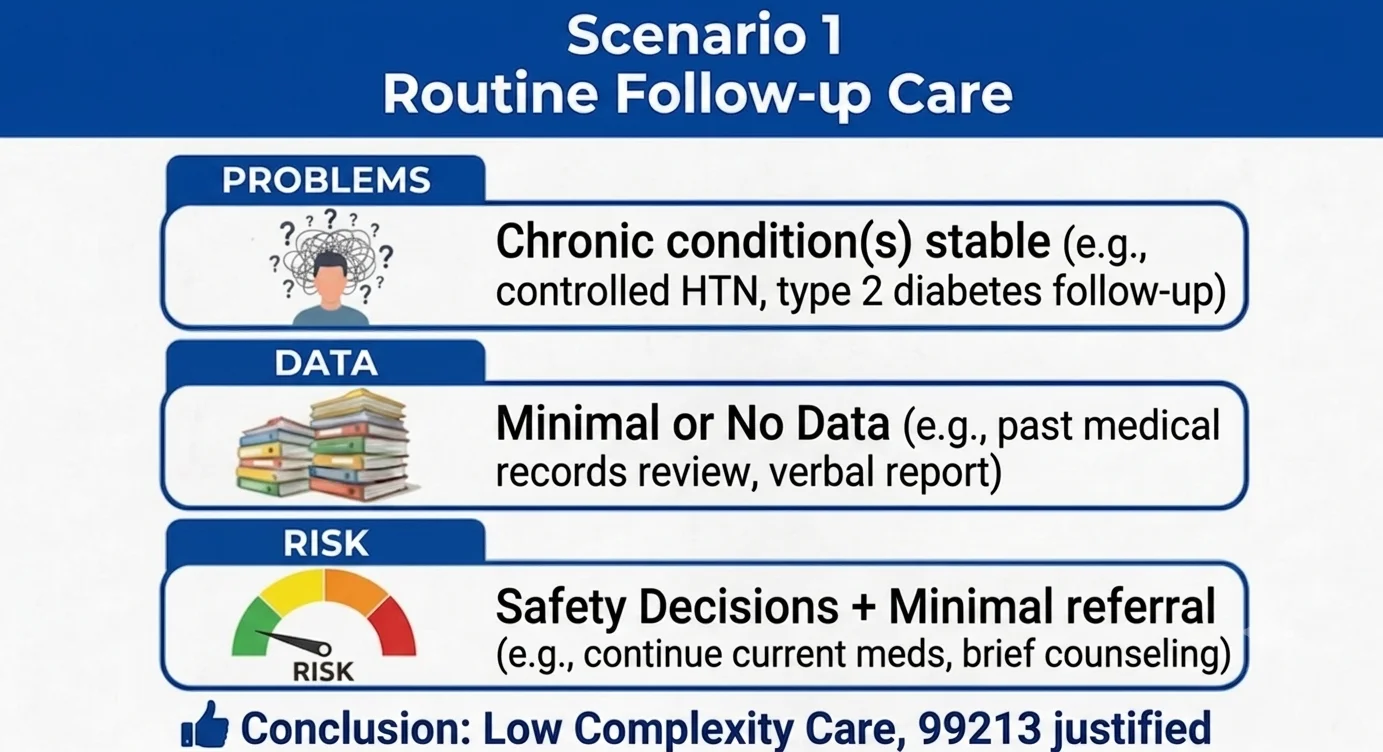
- Management/Risk: The provider titrates the patient’s insulin glargine and adjusts an ACE inhibitor to optimize renal protection. This is a classic baseline scenario frequently built into family medicine billing templates.
Scenario 2: New Acute Neurological or Cardiac Symptoms
A 52-year-old patient presents with new-onset, intermittent unilateral numbness and mild dizziness.
- Problems Addressed: A new, undiagnosed acute symptom that carries a high risk of morbidity if misdiagnosed (Moderate).
- Data Reviewed: The provider reviews an immediate in-office ECG and orders an urgent outpatient brain MRI and carotid duplex ultrasound (Moderate).
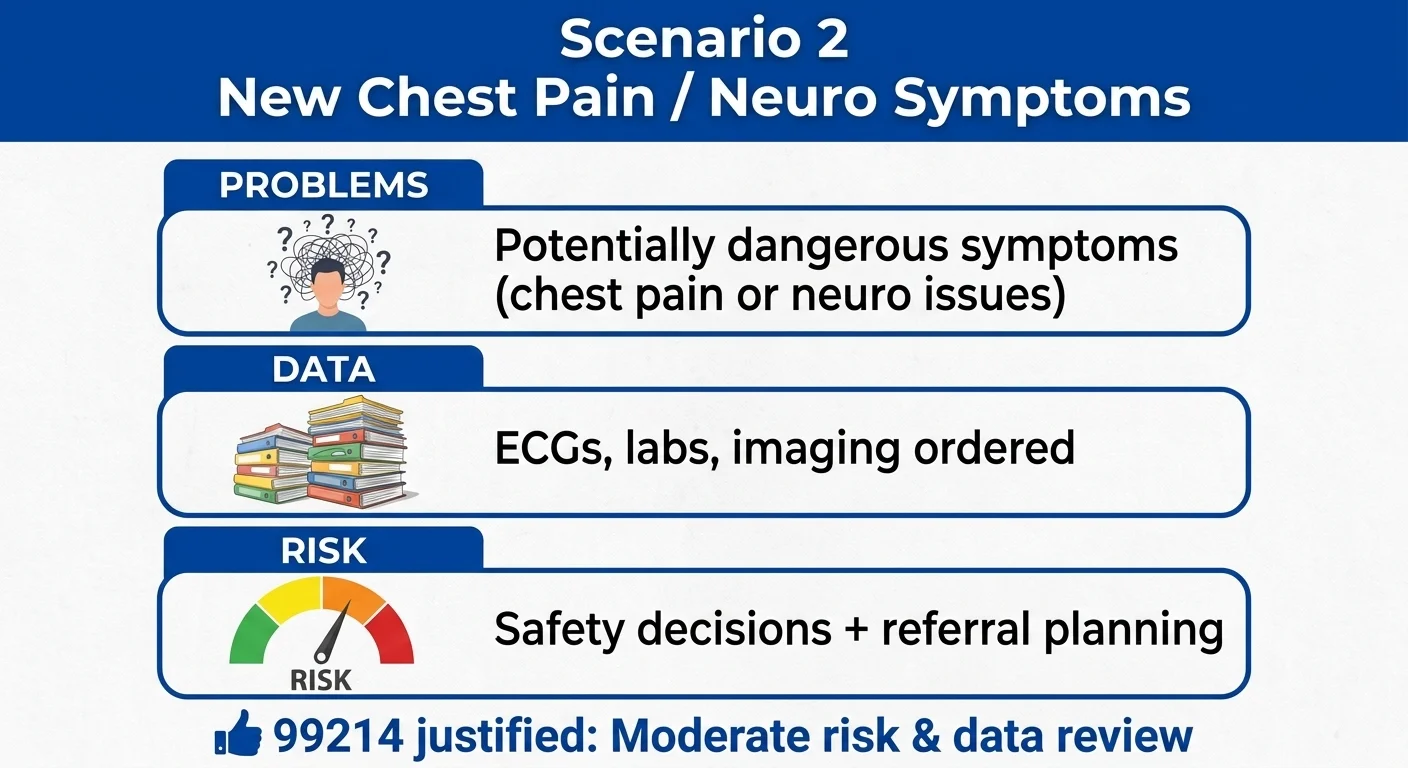
- Management/Risk: The provider establishes a detailed safety plan, outlines emergent red-flag symptoms, and initiates an immediate referral to neurology. Without clear text linking the diagnosis to the plan, insurers may downcode the visit, resulting in an automated co-45 denial code what it means and how to handle it.
Scenario 3: Behavioral Health Integration and Medication Shift
A 35-year-old established patient returns for a follow-up regarding major depressive disorder and generalized anxiety disorder, noting partial response and side effects.
- Problems Addressed: Two chronic conditions that are suboptimally controlled or worsening (Moderate).
- Data Reviewed: Review and scoring of standard PHQ-9 and GAD-7 assessment tools along with prior medication logs (Moderate). This intensive level of tracking fits perfectly within the scope of clinical internal medicine benchmarks.
- Management/Risk: The provider discontinues the failing SSRI, cross-tapers the patient onto a new SNRI, and coordinates a formal referral for psychotherapy (Moderate Risk).
Telehealth and CPT Code 99214 Compliance
Virtual care remains highly utilized, but billing a 99214 for telemedicine requires strict adherence to federal and payer-specific guidelines. Clinical administrative teams can rely on reliable general practice medical billing services by MedicureMD to keep their virtual modifiers updated in real-time.
Audio-Video (Synchronous) Requirements
For standard video telehealth encounters, the clinical complexity (Moderate MDM) or time framework (30-39 minutes) must remain identical to an in-person visit. To secure payment, billing workflows must deploy:
- Modifier 95: Append this modifier to the primary code (e.g., 99214-95) to certify that the service was delivered via real-time, synchronous interactive audio-visual technology.
- Place of Service (POS) Codes: Utilize POS 10 if the patient is residing in their private home during the encounter, or POS 02 if the patient is located at a qualifying healthcare facility. These virtual designations are vital for clean claim processing in everyday family medicine billing.
To ensure accurate and efficient processing, follow these best practices:
-
Document the Modality: Clearly document in your records whether the telemedicine visit was audio-video or audio-only.
-
Adhere to Payer Specifics: Follow the payer’s specific rules regarding the use of modifiers (95, 93, GT, GQ) and Place of Service (POS) codes (02 vs. 10).
-
Maintain an Updated Payer Guide: Consult with your coding/billing department or medical billing company and maintain an updated list of payer rules related to telemedicine CPT code 99214. This will ensure that your initial telemedicine 99214 submissions are clean and paid.
Audio-Only (Telephone) Restrictions
Billing a 99214 via an audio-only telephone link is subject to much stricter scrutiny. Many commercial payers do not consider audio-only equivalent to an E/M code. If a payer does permit audio-only reporting for a level-4 service, you may be required to append Modifier 93 instead of 95. Incorrectly utilizing these codes will quickly produce an unwanted administrative write-off, similar to the scenarios listed in our discussion of the co-45 denial code what it means and how to handle it.
Key Modifiers Utilized with CPT 99214
The accurate application of modifiers is the primary defense against administrative rejections and coding friction inside multi-specialty internal medicine practices.
1. The 25 Modifier Description and Application
The 25 modifier description specifies a “significant, separately identifiable evaluation and management service by the same physician on the same day of a procedure or other service.”
You must append Modifier 25 to CPT 99214 when a provider addresses a distinct, medically necessary E/M issue that goes completely beyond the routine pre-procedural and post-procedural work of a minor procedure performed during that same visit. For example, if a patient presents for a scheduled therapeutic joint injection, but also requires an extensive evaluation and prescription change for an unrelated, flaring chronic illness, the claim should read 99214-25 alongside the specific procedure code.
2. Modifier 24
This modifier is utilized when a provider must perform a 99214 E/M service during the postoperative global period of an entirely unrelated surgical procedure. It alerts the clearinghouse that the evaluation has no clinical connection to the recent surgery. Managing these multi-layered claims is easier when integrating reliable general practice medical billing services by MedicureMD.
3. Modifier 57
This modifier is applied when an outpatient evaluation directly results in the critical clinical decision to proceed with a major surgical intervention within the next 24 to 48 hours. This must be recorded with exact details to bypass automated rejections in standard family medicine billing.
Top Billing Pitfalls with CPT 99214 and How to Avoid Them
Pitfall 1: Undercoding Due to Audit Apprehension
Many practices defaults to coding a 99213 for almost every established patient encounter simply out of fear of triggering an insurance audit. This habit leaves legitimate revenue uncollected.
- The Solution: Build a definitive checklist within your EHR template. If the chart objectively shows that two stable problems were managed and a prescription drug was reviewed, code the 99214 with confidence. For advanced system setups, consult the tech support at reliable general practice medical billing services by MedicureMD.
Pitfall 2: Overcoding Without Complete Documentation
Auditors evaluate claims based strictly on the written clinical record. Reflecting a long, complex conversation in your mind without putting it on paper will trigger a downcode or a recoupment.
- The Solution: Clearly state your parameters. If billing by time, explicitly state the minute count and the exact activities performed. If billing by MDM, ensure the treatment plan clearly links to the diagnosis. This documentation approach is standard across all high-performing internal medicine practices.
Pitfall 3: Telehealth Modifiers and POS Mismatches
Omitting Modifier 95 or pairing it with an incorrect in-person Place of Service code creates an immediate mismatch, triggering common processing disruptions.
- The Solution: Create automated billing rules within your practice management system that automatically link POS 10/02 with Modifier 95 whenever a telehealth encounter template is generated. This is an essential automation feature to implement within your family medicine billing operations.
Pitfall 4: Hidden Complexity and Disconnected Documentation
A provider may execute highly complex cognitive work during a visit, but write a final note that concludes with a vague phrase like “Continue current treatment protocols.” This hides the complexity, leading to an unfair denial or an unexpected co-45 denial code what it means and how to handle it, which indicates an unallowable contractual adjustment due to billing discrepancies.
- The Solution: Explicitly connect the assessment to the plan. Instead of a blanket statement, write: “Diabetes remains stable on current Metformin dosage; checked labs today to monitor renal function before confirming long-term refills.”
Optimize Your Revenue Cycle Today
Prevent coding errors from impacting your practice’s bottom line. Partner with MedicureMD to secure compliant, accurate billing workflows.
FAQ’s
What is the exact time requirement for CPT 99214?
To bill CPT 99214 based on time, the provider must spend and document a total of 30 to 39 minutes of care on the exact date of the encounter.
Can Nurse Practitioners (NPs) and Physician Assistants (PAs) bill CPT 99214?
Yes. Mid-level providers can legally bill for CPT 99214, provided that the service falls within their state’s scope of practice, the clinical documentation satisfies either the 30-39 minute time window or moderate MDM criteria, and all specific payer regulations regarding collaborative oversight are met. Keeping track of these clinical credentials is a primary feature within the reliable general practice medical billing services by MedicureMD.
Can CPT 99214 be fully reimbursed for telehealth encounters?
Yes. The vast majority of major payers, including Medicare and commercial networks, provide full coverage for 99214 via telehealth. The encounter must meet standard documentation requirements and utilize appropriate modifiers (such as Modifier 95) and correct POS indicators, avoiding basic structural mistakes highlighted in our guide on the co-45 denial code what it means and how to handle it.
Can I bill CPT 99214 and a minor procedure on the exact same day?
Yes. You can bill them together if the evaluation represents a separate, distinct, and medically necessary service. To do this properly, you must append Modifier 25 to the 99214 code on your claim form. This requirement is highly common in standard family medicine billing environments when minor skin or joint procedures are carried out.
Does a 99214 encounter always require a comprehensive or detailed physical exam?
No. Under current E/M guidelines, the physical exam and historical review do not dictate the code level. The documentation only needs to show a medically appropriate history and exam. The final code tier is determined solely by Time or MDM complexity. This logic applies to all primary medical specialties, including comprehensive internal medicine operations.
Is there a limit on how frequently CPT 99214 can be billed for the same patient?
There is no explicit frequency limitation built into the CPT manual. You can bill a 99214 as often as it is medically necessary. However, excessive or repetitive utilization for the same patient will attract payer scrutiny, making solid documentation of changing medical necessity absolutely vital. If you need assistance structuring frequent encounters, you can consult with reliable general practice medical billing services by MedicureMD.



